Continuity Of Oral Care Through Communication
 Submitted by Dr. Joy Poskozim DDS, FSCD, CDP
Submitted by Dr. Joy Poskozim DDS, FSCD, CDP
Founder of Joyful Dental Care – House Calls, Advocate, & Presenter
Geriatric House Call Dentist for over 15 years, Dr. Joy Poskozim speaks to Long-term Care Facility Administrators, Nursing Staff, Caregivers, and loved ones on the importance of oral health care as we age. Her goal is to share as much dental information as possible, thereby making it easier to communicate to traveling dentists on what oral health problems residents may have.
Having provided oral care for the geriatric community for over fifteen years, Joy understands medical conditions – and the subsequent issues revolving around them – supersede oral care.
Communication is key to oral health
Communication Within Communities Is Important
 When I get contacted by a Continuing Care Community to see a resident, I try to accumulate as much information as possible to provide the best treatment possible. The Face Sheet is gold in the fact that it usually provides not only the resident’s info and meds, but also the medical and financial Powers of Attorney. These names are crucial in order to make sure everyone is on board for treatment: the Medical POA agrees to the treatment, and the Financial POA will pay for it.
When I get contacted by a Continuing Care Community to see a resident, I try to accumulate as much information as possible to provide the best treatment possible. The Face Sheet is gold in the fact that it usually provides not only the resident’s info and meds, but also the medical and financial Powers of Attorney. These names are crucial in order to make sure everyone is on board for treatment: the Medical POA agrees to the treatment, and the Financial POA will pay for it.
In IL, Medicare does not cover dental procedures. If someone has Medicare Part G, only dental cleanings and exams are covered at all. If someone has dental insurance, we will collect monies in advance and have their insurance pay them directly. All of this info is discussed with the families prior to me seeing and/or treating their loved ones, so all are on the same page.
Communication within the community is also incredibly important. When I am done serving my patients, I always email the Director of Nursing my findings based on the resident’s room number to preserve confidentiality, as I am emailing from my phone.
I also call each family personally at the home based on the responsible party. Sometimes I am calling both the spouse and POA, sometimes I am calling both POAs if there are more than one. I will also write my notes either in their books in the Progress Notes section, or, if I am privy to do so, will input my notes in the software program.
Physicians’ Orders Are Legal Documents
 I use Physician’s Orders (or a POS) when I prescribe prescription-strength Fluoride toothpaste, antibiotics if I see a tooth abscess or severe gum disease, or even when dentures need to be taken out after dinner/put in before breakfast.
I use Physician’s Orders (or a POS) when I prescribe prescription-strength Fluoride toothpaste, antibiotics if I see a tooth abscess or severe gum disease, or even when dentures need to be taken out after dinner/put in before breakfast.
Physicians’ Orders are legal documents, and I let the families know this. Orders are reviewed at shift nursing and caregiving changes.
I will also discuss my findings directly with the caregivers on the floor. A lot of the time a caregiver has been assigned to a wing or group of residents, and I want to make sure they see what I see, bringing them into the room with me if I do see an abscess, loose tooth, bad gingivitis, etc. I will also provide techniques directly for taking a denture out, for example, or brushing their teeth. If I see that a resident is pocketing food after a meal, I demonstrate how to effectively remove these food stuffs in order to prevent choking, and I recommend that this person is seen by a swallowing specialist, if not already done.
Ideally, I am there either after a meal to check on this and to make sure teeth are being brushed, or during a shift change, so I can show/explain to as many staff as possible my findings.
When I do find something that requires antibiotics, I will email the DON and the appointed family members my findings, and the reason(s) behind this is required.
I do not perform anything outside of cleanings/exams until it has been approved by the family or the prescribing physician, if someone needs a tooth removed and they are on blood thinners. I respond to what the physician decides on protocols of stopping a medication if necessary, or adding an anti-anxiety medication if needed to perform a certain procedure.
 Once I have a list of residents I will be seeing that day, the home is called with the list in the hopes of making sure no one is also going to be seeing the podiatrist at the same time, or getting their hair/nails done, etc. These other activities are equally important for their social and mental well-being. I am an asset, and an Independent Contractor, for the community, and I truly loathe breaking up someone’s routine. The worst thing, however, is that the DON may have been informed, but the Activities Director or even the caregiver has not been notified. This happens all the time, and sometimes I do not see the resident as they are already previously engaged.
Once I have a list of residents I will be seeing that day, the home is called with the list in the hopes of making sure no one is also going to be seeing the podiatrist at the same time, or getting their hair/nails done, etc. These other activities are equally important for their social and mental well-being. I am an asset, and an Independent Contractor, for the community, and I truly loathe breaking up someone’s routine. The worst thing, however, is that the DON may have been informed, but the Activities Director or even the caregiver has not been notified. This happens all the time, and sometimes I do not see the resident as they are already previously engaged.
Most of us know this already, but it is good to review:
I prefer to know ahead of time if a caregiver has been given a hard time in attempting to clean teeth, take dentures in/out, etc. This way I can meet with the caregiver and resident at the same time to discuss options in keeping one’s mouth as healthy as possible, despite the potential limitations of the resident and the caregivers themselves. Education is everything. The more we can share our knowledge, the better for the residents’ livelihoods, and less chance of dental emergencies.
We live in a great time for communication! I love getting texts/emails with pictures of crowns that have come out, questions about what a dental abscess looks like (and is this a dental abscess?), or comments stating one of my patients is no longer able to take their dentures out at night – what to do? The more I can help in real time and not have to be onsite for diagnosis and treatment planning the better. Pictures speak a thousand words.
Knowledge Is Power
Knowledge is power, and I want the caregivers to feel empowered by shared information when they take care of their residents’ oral health. Also, repetition is important. Studies show it takes seven times explained in different ways to retain said information. So, when a resident has a new denture to put in/take out, I will first show how to do so if the resident cannot do this themselves, then I have as many caregivers do the same thing I did for the resident. Why? Because shifts change, and not one resident will have the same caregiver every day at the same time. Also, the more that learn how to put in/take out a denture, the more that info can be shared, thus empowering the caregivers who have very little to no dental experience! Communication is key.
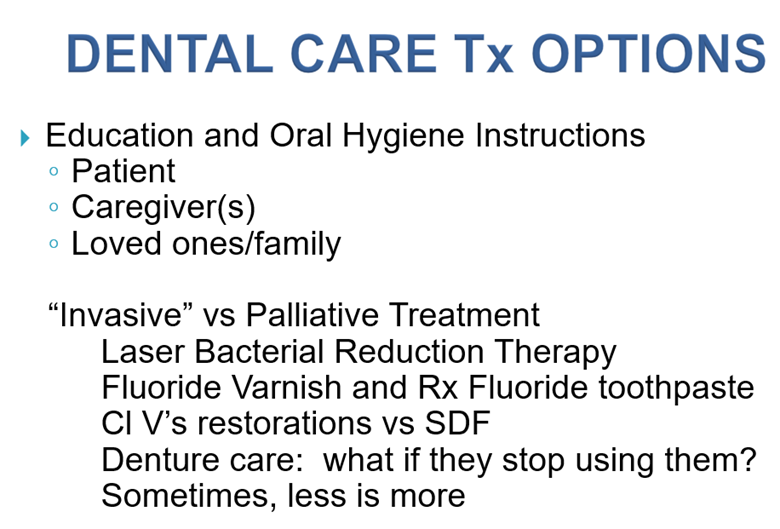
One of my slides that I share at my dental conventions. As a dentist, I usually have options for treatment. And, yes, sometimes less is more. If a resident has decided for whatever reason to stop wearing their dentures, but are not failing to thrive, sometimes this is the hardest conversation I have with the family. Yes, you will have to be seeing them in a different way – without their teeth – but if they are more comfortable this way (not gagging, less chance of choking, cleaner mouth), then it is not how the resident looks to the family, but how the resident feels instead. The resident comes first.
Sometimes I have had a resident whose dentures were lost weeks ago, but said resident is living just fine as is. I explain to the family that we will continue to monitor weight and diet, but, once again, if their loved one is as happy as a clam, I do not feel comfortable charging a lot of money for a new denture if they are not going to wear it anyway, only to be lost again.
This is also true for front teeth that may have fallen out or broken off at the gumline. I seriously had this conversation with a son at a memory care community last week. The son was already aware of the broken-off front tooth, and was, fortunately, in agreement with me that his mom didn’t remember losing the tooth and was perfectly content without it. I explained to the son/POA and the DON that nothing was going to be done about the loss of this tooth. At the end of the day, we were all on the same page.
When Push Comes To Shove
When push comes to shove, I will always choose the palliative over invasive types of treatment for my memory care patients. I explain my reasoning behind applying Silver Diamine Fluoride with a brush over trying to drill into a tooth to remove decay in a tooth. I email both the loved ones/POAs and the DON information on SDF and why I feel it is the better way to go. Once approved by all the powers at hand, only then will I perform the treatment that was agreed upon.
Effective teamwork starts and ends with good communication, mutual respect, and a sense of value of what each one of us brings to the table for the best overall health of our residents/clients/patients/loved ones.
Questions/comments? Never hesitate to reach out!
 Submitted by Dr. Joy Poskozim DDS, FSCD, CDP
Submitted by Dr. Joy Poskozim DDS, FSCD, CDP

Founder of Joyful Dental Care – House Calls, Advocate, & Presenter
Geriatric House Call Dentist for over 15 years, Dr. Joy Poskozim speaks to Long-term Care Facility Administrators, Nursing Staff, Caregivers, and loved ones on the importance of oral health care as we age. Her goal is to share as much dental information as possible, thereby making it easier to communicate to traveling dentists on what oral health problems residents may have.